|
| Pathology Specimens |
On my mission trips, I see a large number of patients with tumors. Most of these patients ultimately require surgery. Surgically removing a tumor is not the end of the work, however. Just like in the USA, it is necessary to determine the type of tumor removed and what additional treatment is necessary. So what do we do with all the terrible tumors we remove in Nigeria?
 |
| Squamous cell carcinoma of the face in an albino patient |
At the end of each case, we cut off a small specimen of the tumor to bring back to the USA. We don't take a specimen from every tumor we remove, just the ones that might be cancer, in order to cut down on costs. At the end of a typical trip, we have about 40 specimens (about one third of the cases). Before I leave, I tell each patient to contact the doctors in the hospital in about 6 weeks in order to get the pathology results. We also have their phone numbers and they have my email.
Next, we have to get the specimens though Nigerian customs. This can be tricky, occassionally. Customs officers have been known, on occasion, to look for problems so that they can get a "gift" to solve it. One time the customs officer opened my box of specimens and demanded to know what they were. I told him they were body parts! He quickly closed the box and waved me through.
 |
| Danny Milner, MD |
Finally, I send the specimens to the pathologist. I am very fortunate to know Dr. Danny Milner, a pathologist at the Brigham and Women's Hospital in Boston. Dr. Milner has been traveling to Africa since 1997 and spent the last 11 years visiting Malawi to work in the Histopathology Department of the University of Malawi College of Medicine. Dr. Milner actively collaborates with clinicians and scientists in Senegal, Mali, The Gambia, Nigeria, Rwanda, and Haiti for both medical pathology support and research efforts. His humanitarian efforts focus largely on creating, expanding, and supporting pathology services in underserved areas through initiatives with the Dana-Farber Cancer Center, Partners in Health, the Harvard School of Public Health, and the Brigham and Women's Hospital.
Dr. Milner is the answer man. He and the Brigham team examine the specimens and determine what we have removed. Then I send the results on to Nigeria and all the patients are contacted. Despite the complexity of the followup, we are usually able to contact almost every patient.
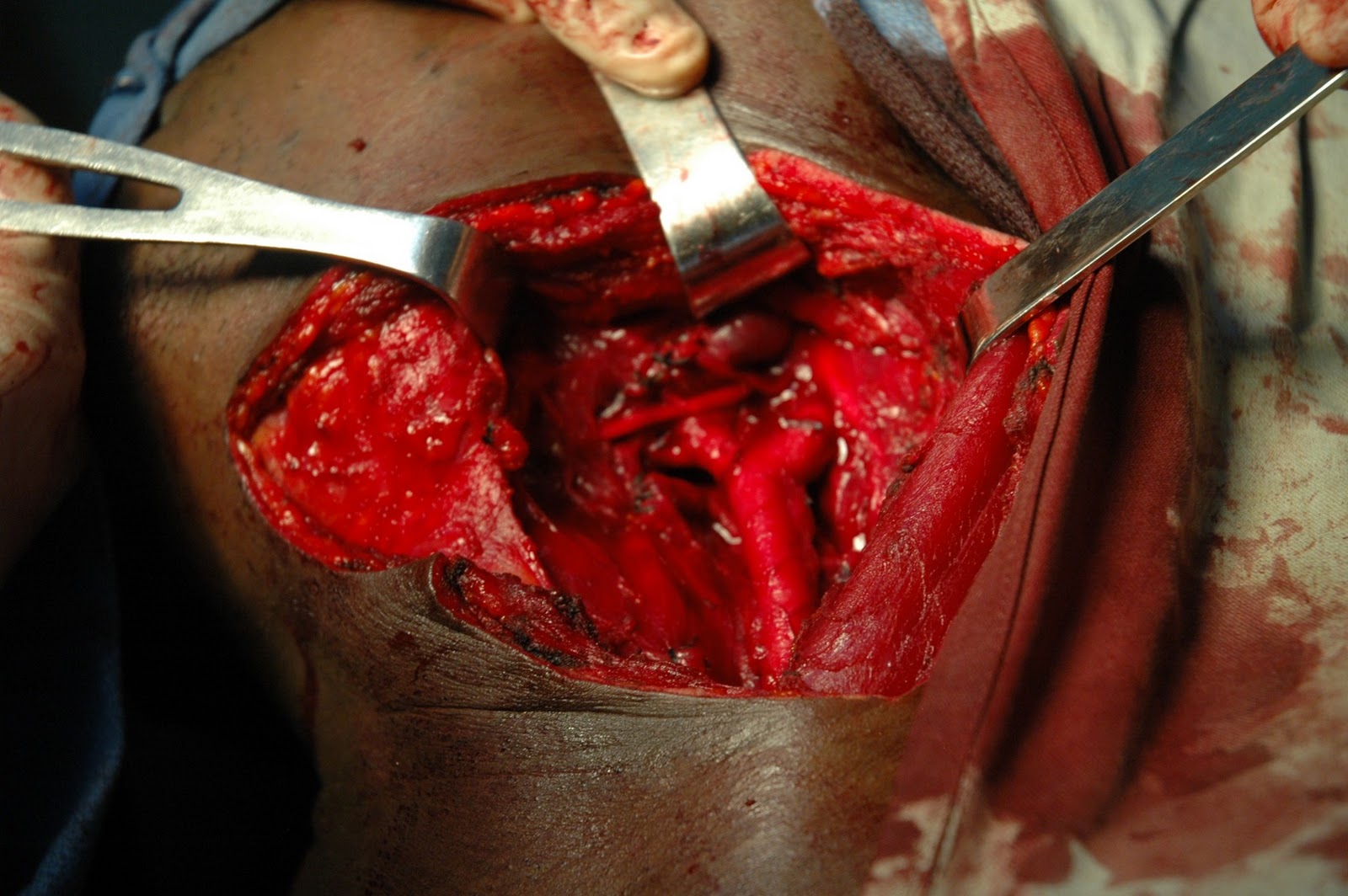
 This lady arrived at the hospital several days before I came. She was told that I was coming and might be able to help her. She was reported to have a recurrent Spindle cell tumor that has been operated on four times in the past-the last surgery being about 1.5 years ago. She has no evidence of metastatic disease so we decided to resect the tumor.
This lady arrived at the hospital several days before I came. She was told that I was coming and might be able to help her. She was reported to have a recurrent Spindle cell tumor that has been operated on four times in the past-the last surgery being about 1.5 years ago. She has no evidence of metastatic disease so we decided to resect the tumor.
 Addendum (10/21/11) : After her big surgery, this patient was not nutritionally well enough to tolerate more operations so we dressed her wound and fed her well. She slowly improved. and her wound started granulating. At the time of my departure she is almost ready for discharge. Dr. Mike has agreed to do a skin graft in the near future.
Addendum (10/21/11) : After her big surgery, this patient was not nutritionally well enough to tolerate more operations so we dressed her wound and fed her well. She slowly improved. and her wound started granulating. At the time of my departure she is almost ready for discharge. Dr. Mike has agreed to do a skin graft in the near future.