We do so many thyroid operations that we occasionally see unusual anatomy such as the non-recurrent recurrent laryngeal nerve. In the case illustrated here, there is a right non-recurrent recurrent laryngeal nerve that we astutely (or luckily) identified. The recurrent nerve branches directly off the vagus nerve rather than taking the recurrent route.The biggest problem with this anomaly is that the nerve can be injured during thyroid surgery.
 |
| Right non-recurrent recurrent laryngeal nerve. (Note that the retraction is pulling the vagus nerve to the patient's right and pulling the trachea to the patient's left) |
 |
| Normal course of the recurrent laryngeal nerves |
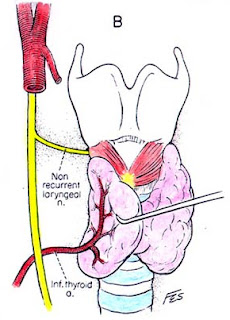 |
| Right non-recurrent recurrent laryngeal nerve |















































